
Improving NHS patient outcomes with data and user-centred design
You’ve seen the headlines. Government services are under more pressure to deliver than ever, with fewer resources, and we all feel the crunch. If you’re a public sector professional, you’re also feeling the relentless pressure to cut costs and justify every spending decision.
Surprise, surprise: this data consultancy says, “Data can help!” The public sector can use data to navigate complexity and make better-informed decisions. It can also commit to user-centred design, which informs what data should be collected and how it’s made available.
The good news is that there are now many vocal advocates of data quality and user-centered design in the public sector. The Government Digital Service’s pioneering guidelines have become a source of best practice in the public sector and beyond for designing in a more user-friendly way.
When the user-centred service and content design principles promoted by the GDS meet strategic data use, it can transform public services. This is where Register Dynamics fits in: we use our data expertise, commitment to user-centred design, and agile ways of working to collaborate with public sector partners to create and streamline effective services. Previous projects include working with the:
Department for Education to use data to reduce teacher shortages
Ministry of Justice to reduce pressure on prisons
Central Digital and Data Office to retain better control of their data.
In this post, we’ll take a quick look at our current ongoing work with the Department of Health and Social Care on their Medtech Compass digital service to help the NHS implement “value-based procurement”. We’ll show how effective data collection and management, user-centered design, and agile working can come together to enable ambitious policy solutions.
The policy vision: value-based procurement
Historically, NHS medical technology (medtech) procurement has prioritised cost over longer-term value based on patient outcomes or sustainability. This cost focus is aggravated by the fact that NHS Trusts may double (or triple, or quadruple) efforts to evaluate products, and that there’s no centralised way to share evaluations or assess the reliability of supplier data. In the absence of clarity, cost becomes the default decisive factor, especially in an extremely budget-conscious environment.
The Government’s 2023 medtech strategy proposed a shift in this approach to medical procurement. In particular, it recommended a focus on delivering value for money across the NHS – specifically aiming to include patient outcomes and system-wide benefits in value-for-money assessments of medical products.
Extracting, mapping, and matching data
To use quality data that gets at longer-term benefits and patient outcomes, procurement professionals need access to quality data. They also need a way to share their own data. Medical procurement professionals can currently consult many disjointed sources of product evidence from other trusts and health organisations, but not all of them are useful. Meanwhile, suppliers submit the same information over and over again because there is no central repository or platform for medical technology evaluations. These information siloes encourage an overreliance on spending data and help drive purchasing decisions that are opaque and not fully informed.
In general, the public sector tends to have lots of data in lots of different places. Finding a way to harness this data to support effective services that are designed for specific user needs is a really exciting application of our expertise at Register Dynamics.
On the Compass project, Register Dynamics has worked with the DHSC on extensive user research to understand the procurement process from diverse user perspectives. What sources of data are available? How are they currently used? What motivates users to share information with each other and what does the process for doing that look like? Getting at the answers to these questions improved our understanding of pain points in the current user journey and guided our data extraction and mapping work.
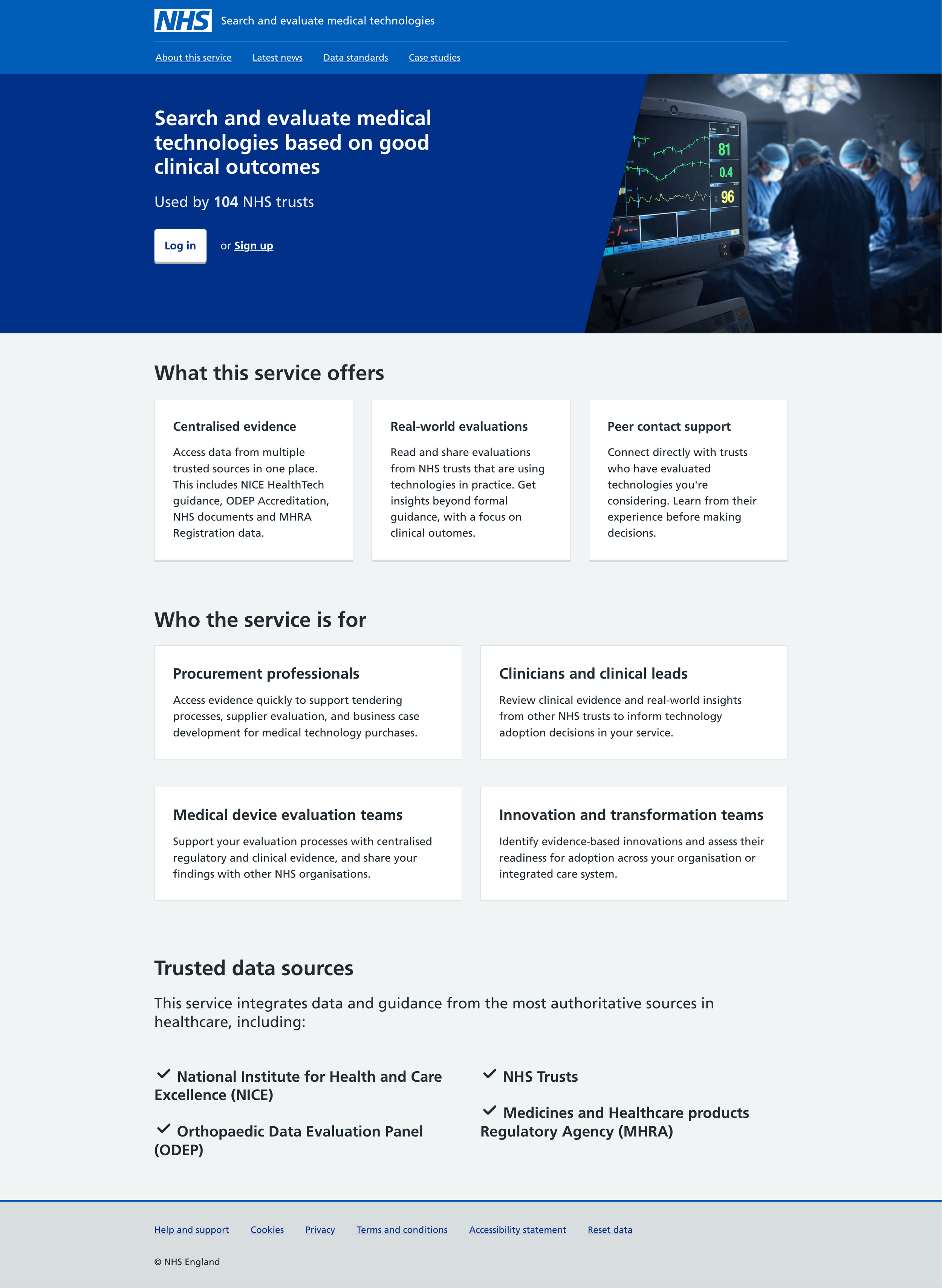
We identified many potentially useful sources of medical product data, including the:
National Institute of Health and Care Excellence (NICE)
Orthopaedic Data Evaluation Panel (ODEP)
National Joint Registry (NJR)
NHS Spend Comparison Service
Medical Devices Outcome Registry (MDOR)
LDEMA (Lots of Data, Even More Acronyms). Part of the challenge in making good use of these data sources is that specific medical products lack global IDs, which means mapping and matching data across sources and services can be complex. Much of the data available is unstructured or requires expert interpretation (for example, a highly technical report or trial), which many users don’t have the resources to manage. Register Dynamics have the specialist data background to find workable solutions to these challenges, including by applying fuzzy matching by product name, category, product code, and supplier, and by developing a human-in-the-loop process for reconciling unconfident matches.
It’s clear that there’s a lot of evidence available to help realise the NHS’s value-based procurement dreams! But even clearer that it needs to be assessed, organised, and centralised. Understanding the opportunities and limitations in each data set means we can help build an effective data-sharing platform. We can use the knowledge we’ve gained from users to decide what data should be used to compare products in the service prototype.
As we continue to work with teams around DHSC, we’re pulling together a data strategy that will make it easier to do more rigorous, value-based medtech procurement. We want to make sure that procurement professionals can (and will!) use the service to share their experience of engaging with medical suppliers and find out how other trusts are making their procurement decisions. This calls for…
User-centred design
We can make sure that the service is something people will actually use by… drumroll… talking to the actual users and applying user-centred design best practices to ideate and iterate.
User research and a focus on user needs informs our work with data sources. It also drives the design of the digital service prototype. Ultimately, the service will pull from and display the data that an individual user wants to see, plus provide essential contact information and tools for sharing their own medical product evaluations and experiences.
We’ve run user research sessions with people in various procurement roles, as well as clinicians, and will soon speak to suppliers. These sessions test the structure, functionality, and language of the design prototype. We want to find out whether users are confident they can access the data they need, how they know they can trust what they find through the service, which embedded features and resources excite them the most (or least!), and at what stages of the procurement journey they expect they’d use Compass to find and compare medical technology evaluation data.
Do people understand and like the filters they can apply to the medical product evaluation search results? Do they agree that the service name describes what the service actually does? Is it clear to users what they’re meant to do when they first visit the landing page for the service? Do the colours make them want to throw their computer out the window? These are all questions we need to answer as we work towards each iteration of the prototype.
An important insight that’s come out of user research is that the original data sources we identified are actually less important to medical procurement professionals than we expected. Many users struggle to interpret the highly specialised clinical documentation available from these central data sources and end up relying more heavily on their personal network of peers across NHS trusts for information-sharing. There’s great value in the information held locally by trusts, information that is not always represented in those central data sources.
This finding inspired us to pivot slightly, reorienting our service toward facilitating data sharing between trusts. We designed a way for trusts to upload their own evaluations (including anything from clinical trials to business cases to informal notes) alongside contact details for trust members willing to talk about their experience with the associated medical technology. Users responded enthusiastically to this update.
The most perfect data resources in the world won’t produce an effective service if the user experience is painful or doesn’t reflect the reality of their needs. Good data is a key ingredient in good decision-making, and good user-centred design helps make that data accessible and easy to use.
Bringing it all together with agile working
Agile ways of working empower us to collaborate effectively with the DHSC team. Splitting work into short sprints, we can easily update and retest prototypes based on each new set of data findings and user research insights.
Frequent contact means we can work transparently and nimbly. We can test risky assumptions about user behaviour – for example, assumptions about how users decide evaluations are trustworthy, and whether users will be able and willing to share their own evaluation data – and adjust our strategy for data-driven behavioural change as we learn.
We hope that this new service will help make value-based procurement a reality. It’s a transformation with positive implications for the UK medtech industry and environmental targets. Most importantly, it has the potential to have a real impact on the lives of patients and their families.
Our work with DHSC is just one example of how we collaborate with public sector partners to solve complex, whole problems for users working to implement transformational policy. Good policy can change lives. But it can’t exist without access to good data, and neither can exist without a focus on user needs.
Learn more about how we work with public sector clients in our case studies area.
Author

Tags: